
CLICK TO SHOP OUR BLACK FRIDAY SALE!
*Excludes BioNude and subscriptions
The article “Update in Female Hormonal Therapy: What the Urologist Should Know” by Nirit Rosenblum (NYU Case of the Month, December 2020) is, at its core, a polite but firm reminder to urologists that not everything is a “bladder problem.” Sometimes it is a hormone problem wearing a very convincing disguise. As estrogen levels decline, the entire genitourinary system shifts, and what shows up in the clinic as urgency, frequency, or recurrent infections is often rooted in hormonal depletion rather than simple mechanical dysfunction.
Rosenblum reframes these symptoms through the lens of genitourinary syndrome of menopause (GSM), emphasizing that this is not a niche gynecologic issue but a chronic, system-wide condition that urologists are seeing every day, whether they realize it or not. The takeaway is clear. If you are treating postmenopausal urinary symptoms without considering hormones, you are likely treating the symptom while overlooking the cause.
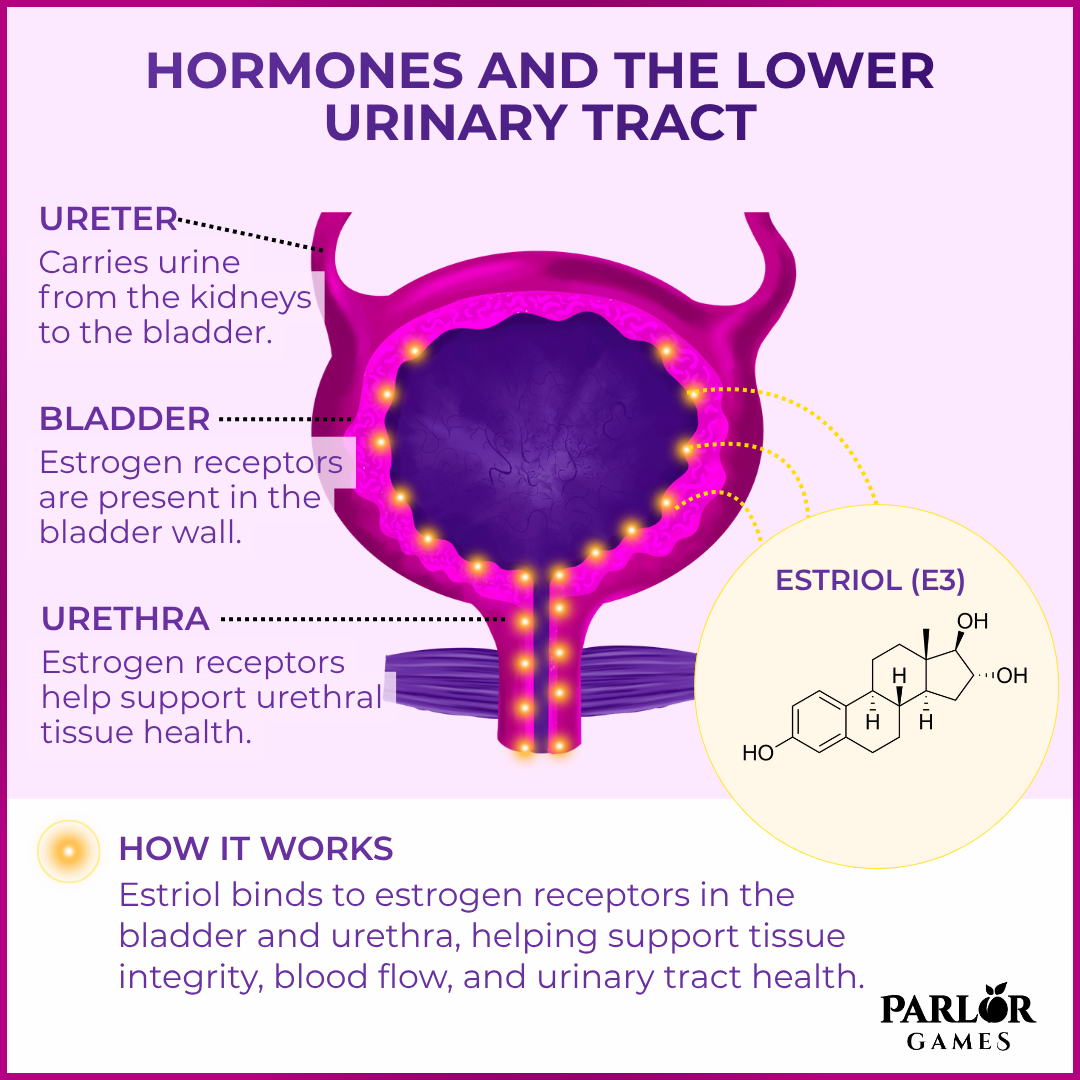
The article explains that estrogen receptors are present throughout the lower urinary tract, including the bladder, urethra, and surrounding pelvic tissues. When estrogen levels decline during menopause, these tissues undergo structural and functional changes. There is thinning of the epithelium, decreased blood flow, reduced collagen content, and diminished elasticity. These changes contribute directly to symptoms like urinary urgency, frequency, dysuria, and recurrent urinary tract infections.
Importantly, the paper emphasizes that these are not isolated gynecologic issues. From a urologic perspective, they affect bladder function, urethral closure pressure, and the overall defense mechanisms of the urinary tract. This is why postmenopausal women often present with what appears to be “chronic UTI” or overactive bladder, when the underlying issue is actually hormonal.
The article frames GSM as a chronic, progressive condition rather than a temporary inconvenience. Symptoms include vaginal dryness, irritation, dyspareunia, urinary urgency, frequency, and recurrent infections. Unlike vasomotor symptoms such as hot flashes, GSM does not resolve over time and often worsens without treatment.
Rosenblum highlights that GSM is underdiagnosed and undertreated, partly because patients may not volunteer symptoms and clinicians may not connect urinary complaints to hormonal decline. This is particularly relevant for urologists, who may see these patients first for bladder-related symptoms rather than vaginal or sexual concerns.
A central focus of the article is the role of estrogen therapy, particularly local (vaginal) estrogen, in managing GSM and associated urinary symptoms. Local estrogen is shown to restore the integrity of the vaginal and urethral epithelium, improve blood flow, and normalize the vaginal microbiome, which in turn reduces infection risk.
The article distinguishes between systemic and local estrogen therapy. Systemic therapy may be used for broader menopausal symptoms, but local estrogen is emphasized as highly effective for urogenital symptoms with minimal systemic absorption. This makes it a preferred option for many women, including those who may not be candidates for systemic hormone therapy.
From a urologic standpoint, local estrogen has been shown to reduce recurrent urinary tract infections, improve symptoms of urgency and frequency, and enhance overall urinary tract health. The mechanism is not just symptomatic relief but actual tissue-level restoration.
Rosenblum addresses common concerns about estrogen therapy, particularly safety. The article notes that low-dose vaginal estrogen is generally considered safe for most women, including many with contraindications to systemic hormone therapy, though individual risk assessment is still necessary.
The paper also stresses the importance of patient education and individualized care. Many women discontinue therapy prematurely or never start it due to fear or misunderstanding about hormones. Clinicians are encouraged to discuss risks and benefits clearly and to consider hormonal therapy as part of a broader management plan.
The key message of the article is that hormonal decline plays a central role in many urologic complaints in postmenopausal women, and ignoring that piece leads to incomplete care. Urologists should actively consider GSM in their differential diagnosis when evaluating urinary symptoms and should be comfortable discussing and prescribing local estrogen therapy when appropriate.
Rosenblum’s update ultimately reframes common urinary complaints not just as bladder problems, but as hormone-driven changes in tissue health. Recognizing this connection allows for more effective, targeted treatment and significantly improves quality of life for affected women.
You can see the full study here: https://pmc.ncbi.nlm.nih.gov/articles/PMC8058921/
Lorem ipsum dolor sit amet, consectetur adipiscing elit.
Lorem ipsum dolor sit amet, consectetur adipiscing elit.
Lorem ipsum dolor sit amet, consectetur adipiscing elit.
Lorem ipsum dolor sit amet, consectetur adipiscing elit.
Disclaimer: The information provided above is intended for educational and informational purposes only. Statements made have not been evaluated by the FDA nor are they intended to treat or diagnose. Any health concerns should be discussed and evaluated by your primary health care provider.
Parlor Games, LLC ● kate@parlor-games.com ● 5304 River Rd N Ste B ● Keizer OR 97303
Disclaimer: The information provided above is intended for educational and informational purposes only. Statements made have not been evaluated by the FDA nor are they intended to treat or diagnose. Any health concerns should be discussed and evaluated by your primary health care provider.
28 Day Challenge Subscription Details

We ship you a 28 day supply of Silky Peach Cream for only $29 (more than 25% off our normal price) when you sign up for Subscribe & Save.
Follow the directions we include in the package and apply Silky Peach cream on your tender bits for 28 days.

Decision Day:
5 days before your subscription rebills, we’ll send you an email reminder with a link. If you decide Silky Peach is nice but not your thing… you can click that link and cancel your subscription without even talking to anyone. No hassle — no questions asked.
If you are like 72% of our Silky Peach customers, you’ll love it and can't imagine life without it. In that case, do nothing, and we’ll welcome you to the Parlor Games family and ship Silky Peach Cream to your door step every month for the same discounted price of $29 — locked in for as long as you remain a subscriber.

Important note about our easy-breezy subscriptions:
We know that some companies make it hard to cancel a subscription — that’s not us. Our mission is to save the world — one vagina at a time! If you decide you don’t need Estriol as an ongoing solution for dryness, incontinence, UTIs and keeping sex fun and comfortable again, we understand. Five days before we ship your next order, you'll receive an email with a link to cancel right there in the message.
No hunting, no searching, we got you. Respect is where it’s at.
FYI – Estriol is beneficial for skin integrity and mucous membranes. It’s great for vaginal atrophy and also amazing for use on the face and neck. Applying a small amount — about 1 pump — can help build the collagen and plump up the cells to reduce wrinkles. Who knew!!
OUR HAPPINESS GUARANTEE
We want you to feel safe and confident trying any of our products. That's why we promise 100% money-back guarantee on the purchase price of the first bottle of any of our products. Balancing hormones DOES take some time, so please try it for 28 days. If after 28 days you are unhappy, or the product just hasn't worked for you, simply contact us and we'll process a refund of your full purchase price upon receipt. Sorry, shipping fees are not refundable.
